Last Saturday was World Hearing Day, so I showed a few shots of my Bionic Ear on instagram. Some people were shocked to see I had one! So I decided it was time to do a little updated series here about why I have one, how I got it, how I like it, and what life is like with one. Here's part one.
So, what the heck is a CI, and how does it work?

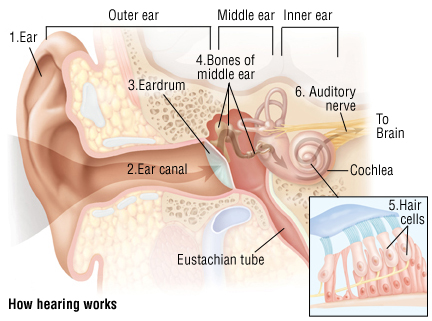
I'm going to keep this really basic. I'm not an audiologist and I don't play one on TV. But this handy chart should help. You see the external bit, but yes, there are things in my head other than my brain. There's the magnet, to hold the processor on, and there's the wire that goes into the cochlea. Remember that the reason my hearing sucks is because my hair cells are dead. The hair cells live in the cochlea. So the wire replaces them, in a sense. The wire has an "array"--I think mine has 24--of sound things. I know that's super technical. I forget the real name. But there are24 different entries on that wire that can be individually fine-tuned. (More about that later) So instead of hundreds of hair cells...I have 24 electrode arrays. Now, it's better than nothing! But I note this to illustrate that CIs are not perfect replacements for real hearing.
I had my surgery in May of 2008. Post transplant I had a lot to deal with--I had a skin graft surgery that November, and then we had to try hearing aids first, and then I had to get myself to agree to having a CI, and so with all that, it was a long-ish process to actually getting one.
The one great thing is that I was "post-lingual"--meaning, I knew how to talk. (Boy howdy, can I talk.) If you have had severe hearing loss for a long time, or if you're a baby getting one, then there's hearing therapy involved. Even now, there are sounds I hear and it takes me a minute to figure out what it is. (While writing this, with my CI on, I heard a crazy loud, scary noise. What is that?! It took me a few seconds, but I figured it out--crows.) Everyone knows the person who is hard of hearing who speaks loudly because she can't hear herself. I can hear myself. I'm just loud. (There are times when I can't hear myself as well--when I have the telecoil on, for example, so in church.)
My ENT is fabulous. I've had him for years--he works a lot with CF folk, and more and more CF folk are having CIs put in. (ENTs also do all our sinus work. We have a lot of sinus work...I am lucky in that area. My sinuses tend to behave.) If you're in the central Ohio area, Dr. Willett, Ohio ENT is my guy and I adore him.
So the day of surgery was just like any other surgery. Port accessed. Ready to rock and roll. You stay over night, of course, because people are putting things in your head! My audiologist, who is also at Ohio ENT, actually stimulated the CI during surgery to make sure it "worked" and that it had been put in correctly. That's a key part of the process, because I didn't get to attach the processor for a month, due to healing. You don't want to attach the processor and have it not work!
For 21-30 days, your head heals. I wore my hearing aids, and waited for activation day. This is the day you see when those videos are posted to Facebook or YouTube where a kid or someone hears for the first time. Mine was not that dramatic. But instantly, small sounds came back--the sound of the turn signal, typing, things like that.
(When your hearing goes, it's usually the upper registers that go first--high notes, high voices, likes kids and women. And fainter sounds, like turn signals, things beeping, etc.)
My audiologist then programmed the CI. You can have up to four programs. Again, I don't want to get super technical, but I have all four slots on my CI filled with programs. There's a tiny button on the processor that I hit to cycle through them. The first is my "normal" program. That allows sound in from all sides, and is good all-purpose. The second is focused on who is directly in front of me, and cuts out side noise and background noise to an extent. This is good for noisy places and restaurants. I have another program that focuses this even more. The fourth program is a richer program that's generally for music, but I can use it as an everyday program, too--you get a wider range of sounds and frequencies.
There is also the telecoil. This cuts out all sound except what you hear through the telecoil system, which lets in whatever's coming in through a microphone.* This is what I use in church, and it's amazing. It's like someone is speaking distinctly and clearly into my ear. You are also, supposedly, able to use this for the phone. That is not my experience. (More on that later.) Of course the issue with the telecoil is that the other person has to have the microphone on, or the system is useless. (It does work for lecterns, too, or stand microphones.)
Now, I have one implant. I don't have one in my right ear, because I want that 20% of real hearing that I have. When a CI is implanted, it removes any residual hearing you have left. I am truly deaf in my left ear without it. But I don't wear my CI all the time, so I need some residual hearing. This allows me to hear my alarm clock and other loud noises. There are also times when the batteries will inexplicably die. (This happened a lot with my first processor, not so much with my current one.) The 20% also helps out my CI, in a sense. It gives me some sense of directionality--where a sound is coming from, although not a lot. When I'm swimming, I can hear loud things. If I know your voice REALLY well--meaning, you're my parent or my best friend or my sibling--then I can decipher what you're saying, sometimes, with just my right ear.
I use rechargeable batteries in my CI. I have three of them, and I rotate them. They get put in and can last about 15-24 hours on a full charge. I tend to not put my implant in early in the morning, because I sort of like the silence. But that's changing as I switch my workout routine to being in the morning. I need to hear the video.
I'm using "hear" here, but what I really mean is "understand". I can hear lots of things. That doesn't mean I understand them, or process them. For example, I heard the crazy bird sounds this morning, but I had no idea what it was.
Also--and I'll talk about this more in the next piece--but everyone's CI experience is very different. Rush Limbaugh has a CI, and he said he can't learn new music. I can, because, as we saw, I was very musically inclined and my ears had been trained that way. My brain still knows that language, in a sense. I work hard to learn new music. Instrumental music is difficult because it all sounds like noise, at first. But I can learn new songs and new vocal pieces with the CI--I just have to approach it differently. Some people with a CI can use phone adaptation stuff. I can't. I don't know why. But more on that next.
*The telecoil can be "mixed"--basically, you can determine how much sound you want to get through the telecoil. Mine is 100%, when it's turned on. But you can do 50/50, 75/25, 90/10....whatever.